





MLTSS cannot succeed in California without integrating assisted living facilities.
By Jason Bloome
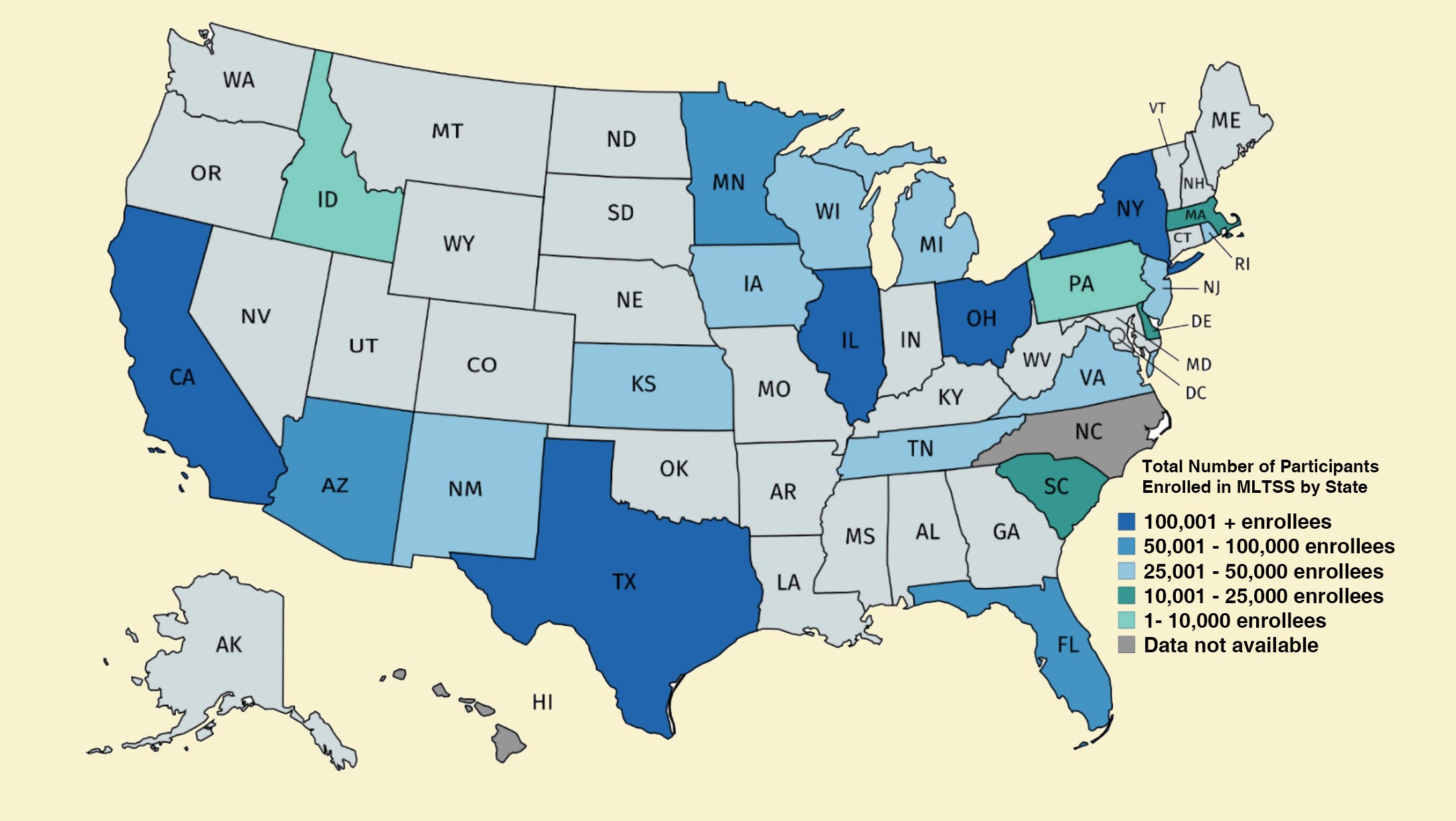
Managed Long Term Support and Services (MLTSS) programs are quickly expanding throughout the nation. More than 24 states have MLTSS programs which consist of State Medicaid Agencies providing capitated payments to managed care organizations (MCOs) for the provision of LTSS, often in addition to other services. LTSS includes services and supports for individuals with functional limitations who need assistance with activities of daily living, including dressing, bathing and help out of bed.
States implement a variety of MLTSS programs, including those that focus primarily on LTSS, comprehensive programs that provide most or all Medicaid services, and fully integrated programs which include all Medicare and Medicaid services. Total enrollment in nationwide MLTSS programs doubled from 800,000 in 2012 to 1.8 million in 2017. The majority of MLTSS recipients are the elderly. The population with the highest needs for LTSS, seniors who are 85+, is projected to triple (a 208% increase) between 2015 and 2050.
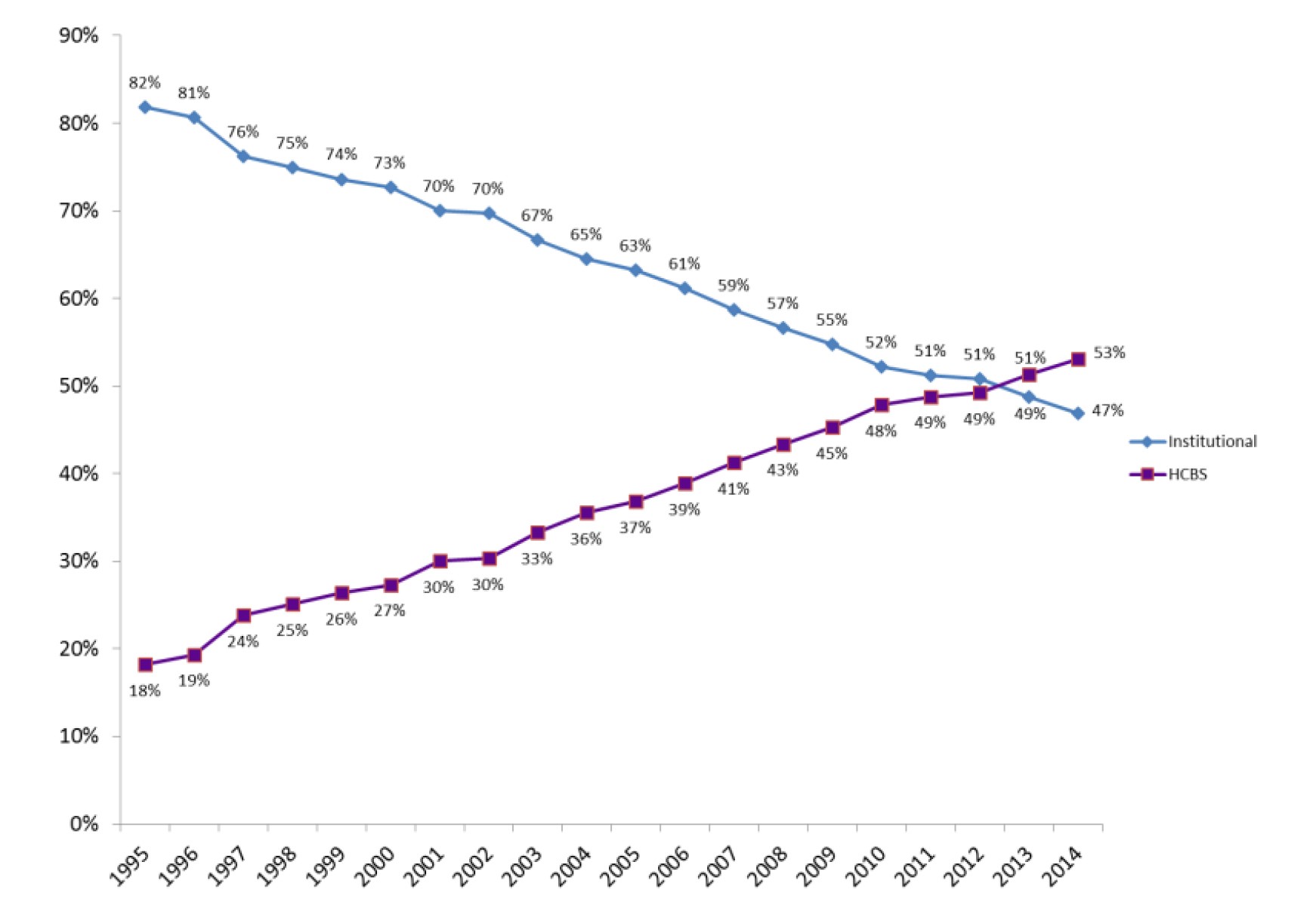
Primary goals of MLTSS programs is to (1) rebalance care from skilled nursing facilities (SNFs) to home-and community-based services (HCBS), (2) provide incentives for high quality care, and (3) control cost growth. As MLTSS programs mature, the proportion of HCBS vs. institutional spending has increased nationwide. In 2016, Medicaid spent an estimated $167 billion on LTSS: of that amount, 57% — or $94 billion — was spent on HCBS.
Assisted living facilities (ALFs) are a critical component of HCBS and necessary for MLTSS rebalancing. Low-income seniors who require too much care to remain at home but who do not need institutional care are ideal candidates for ALFs. Small 4–6 bed ALFs with high staff to resident ratios provide safe care settings for many elderly who require 24-hour custodial care (e.g., require help with dressing, bathing, have incontinence, are in wheelchairs or have dementia and could “wander”). Since providing care in community-based settings is usually far more affordable than institutional care, LTSS rebalancing to ALFs save Medi-Cal dollars.
Of the six states with the largest number of MLTSS enrollees five already integrate or will soon integrate ALFs into their MLTSS programs.
In New York, by January 2019, all assisted living waiver programs will be fully integrated into its MLTSS program. In Florida, ALFs were rolled into its Statewide Managed Medicaid Program in 2013. In Texas, all assisted living waiver services were rolled into its Star-Plus program in 2014. In Pennsylvania, by January 2019, the Community HealthChoices Program, which continues MLTSS integration throughout the state, includes ALFs. In Ohio, ALFs are included in the MyCare Ohio MLTSS plan.
Absent from this list is a state with one of the nation’s largest number of MLTSS enrollees: California. As of December 2018, California had no provision to integrate ALFs into its MLTSS program.
California’s MLTSS plan, called the California Coordinated Care Initiative (CCI), has had serious growing pains since it began in 2013. The Governor’s 2017–2018 budget found the plan to be fiscally unviable; it suffers from a very low opt-in rate for dual-eligible participants who choose to have their Medicare benefits managed by the same CCI MCO that manages their Medi-Cal benefits; and care at home, through the In Home Support and Services (IHSS) program, was dropped from CCI as a managed care benefit.
A capitated rate structure that does not include ALFs and the carve-out of the Assisted Living Waiver (ALW) program is a critical problem at the heart of CCI which results in perverse fiscal incentives that reward CCI MCOs that place seniors into SNFs (by fully reimbursing them for SNF expenses) and punish them when seniors choose to reside in ALFs (by failing to cover the expenses). California’s MLTSS is headed in the wrong direction when instead of promoting affordable ALFs it forces seniors into expensive SNFs when they do not need to be there.
It is time the California Department of Health (DHS) redesigned CCI to include ALF integration. Program changes submitted by DHS to the federal Center for Medicare and Medicaid Services would allow CCI MCOs to develop pilot programs that would encourage LTSS rebalancing from institutions to ALFs for dual-eligibles who choose to reside in those settings. Pilot program successes, once measured, would allow ALW to be ended with current enrollees integrated into ALF managed care programs.
Ideal ALF integration with CCI components would:
- Produce Medi-Cal cost savings by transitioning seniors on LTSS from expensive SNFs to more affordable ALFs.
- Contain costs for SNF-ALF diversion by targeting a subset of Medi-Cal beneficiaries already on IHSS who meet clear and consistent SNF level-of-care eligibility criteria (e.g., who currently receive between 195 and 283 IHSS care hours per month).
- Provide fiscal incentives to CCI MCOs for LTSS rebalancing by establishing a Medi-Cal cost-recovery pool divided between the state and MCOs.
- Utilize MCO case managers to evaluate SNF diversion/transition candidates on a case by case basis and do away with minimum SNF stay requirements (e.g. not every senior who goes to SNFs for rehabilitation should be required to have a 90-day minimum stay in order to be eligible for LTSS services and SNF transition).
- Include participation by seniors who have a Medi-Cal share of cost and/or are at or below three times the poverty level (e.g., receive up to $2,250/month — the current standard used by New York, Texas, Florida, Pennsylvania and Ohio).
California should be the trendsetter in the nation when establishing progressive MLTSS rebalancing programs that shift care from institutions to home-based ALFs. The purpose of CCI was not for the state to save Medi-Cal dollars by forcing MCOs to ration care but to promote cost efficiency by allowing managed care organizations to their job: manage the care along the entire care continuum (from home-ALF-SNF) for seniors eligible to transition from one care setting to another. A puzzle cannot be completed when pieces are missing from the box. Smart MLTSS rebalancing programs requires including all of the critical components, included ALFs.
RESOURCES
https://innovation.cms.gov/Files/reports/fai-ca-firstevalrpt.pdf
https://www.gao.gov/assets/700/694174.pdf
https://www.medicaid.gov/medicaid/managed-care/downloads/ltss/mltssp-inventory-update-2017.pdf
http://www.wnylc.com/health/entry/150/
https://hhs.texas.gov/services/health/medicaid-chip/programs/starplus
http://www.healthchoices.pa.gov/cs/groups/webcontent/documents/document/c_237795.pdf
https://medicaid.ohio.gov/Portals/0/Initiatives/MLTSS/MLTSS_FAQ.pdf
https://innovation.cms.gov/Files/reports/fai-ca-firstevalrpt.pdf





