A version of this article was published in The Crime Report http://thecrimereport.org/2016/11/01/the-misery-of-solitary-confinement/
Last month, New York City Mayor Bill de Blasio announced that solitary confinement will no longer be applied to inmates aged 21 and under who are held in city jails. That’s welcome evidence of the growing recognition of the grueling nature of this punishment.
A standard practice in jails and prisons nationwide, solitary confinement is used to punish jailhouse infractions, although it can also be used for other purposes, such as securing a high profile inmate, or separating suspected gang members from the general population.
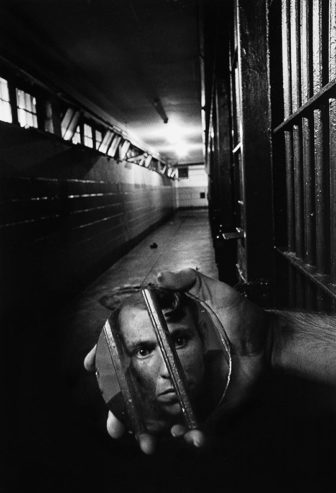
Solitary goes by many names – Administrative Segregation, Special Housing, the SHU, the Box, the Hole, and on Rikers Island, by the slang name, the “Bing” – but it all amounts to the same thing: 23 hours inside a cell roughly the size of a parking spot, no meaningful human contact, with a food tray passed through a flap in the door.
The length of time in the cell can range from a few days, to a few months, to many years.
“If [inmates] had no mental health issues before they entered solitary, they do now.”
As a former assistant chief of mental health in the Rikers Island 500-cell solitary confinement unit, the misery of solitary is something that I knew all too well. Our team was routinely summoned to cell doors to assess those who were threatening suicide, showing signs of psychosis, or making suicidal gestures.
“If they had no mental health issues before they entered solitary, they do now,” was our mantra.
As I took in these grim cells—the cot, the tiny sink and toilet, the small footlocker, and the desperate person inside begging for a reprieve—I was continually struck by the cruelty of this punishment. But as I stood in those doorways, I was also struck by the role I played in this punishment as a mental health caregiver.
A mental health team in a correctional setting provides emotional and psychiatric support to the incarcerated, and especially in a solitary confinement unit. Under the rigors of solitary, mental deterioration is swift, and mountains of anti-depressants, anti-psychotics, and sleeping pills are routinely dispensed.
Yet nothing could have prepared me for blood-smeared cells, makeshift nooses, and agonized shell-shocked faces. My immediate reaction was that this punishment had all the signs of torture, but I brushed the word from my mind.
I was surrounded by all the earmarks of legitimacy: nurses and board-certified doctors in white lab coats, correction officers in navy uniforms, even the American flag flying above the jail.
How could any of this be wrong?
This was a legally sanctioned punishment carried out in jails and prisons across a nation that prides itself as progressive on human rights. Yet despite my rationalizations, whenever I approached a cell door, my knees wobbled, my throat clenched, and I could never seem to get the word torture out of my mind.
Although it has been more than a decade since I left Rikers, I have not forgotten the misery of this unit. I am relieved to see that, with the national spotlight focused on mass incarceration and its related issues, solitary confinement is finally being exposed for the horror that it is.
Pope Francis, President Obama, and Supreme Court Justice Anthony Kennedy have denounced it, while Juan Mendez, the United Nations Special Rapporteur on Torture, has deemed that anything beyond 15 days in solitary constitutes torture.
Some 80,000 to 100,000 people continue to be held in isolation cells in prisons and jails across the country.
With the tide starting to turn, we are seeing the beginnings of reform, primarily in dealing with justice-involved juveniles and the mentally ill. But it is far from enough.
The practice of solitary confinement is deeply entrenched across the nation. Some 80,000 to 100,000 people continue to be held in isolation cells in prisons and jails across the country.
The growing consensus that solitary confinement is inhumane and torturous is apparently, and unfortunately, not shared by the National Association of Social Workers and the American Psychological Association. Yet their members are on the front lines of this issue.
It is social workers and psychologists who enter these cells on a daily basis to assess the mental deterioration that solitary will induce, and to determine when the risk of suicide is high enough to warrant a “timeout.” They are a key component in this punishment; without their participation, solitary confinement as we know it, would come to a halt.
With the United Nations opposing this punishment, and world leaders condemning it, there can be no further ambiguity as to the human rights violations posed by solitary confinement, and no excuses for the “helping professions” to remain silent.
It is time for the National Association of Social Workers and the American Psychological Association to take a meaningful stand, and offer guidance to the thousands in their ranks who, in the course of their duties, are often called upon to be monitors of human suffering.
To do anything less represents a betrayal of the ethics that are at the core of these helping professions.
Mary Buser was a clinical social worker in the Mental Health Department on Rikers Island between 1995 and 2000. She served as assistant chief of Mental Health in the island’s Mental Health Center, as well as the 500-cell Punitive Segregation Unit. Her book, “Lockdown on Rikers,” (St. Martin’s Press) was published in September, 2015, and won the 2016 Brooklyn Eagles Literary Award for non-fiction. She is also a member of Social Workers Against Solitary Confinement. She welcomes comments from readers.
Text reads “DisAbilities Council Virtual Meeting. May 16. 7 – 8:30 PM PT. Virtual” The…
Text reads "Opinion. Clinical Intuition: Another Look" While we are proud to feature opinion pieces…
Text reads "SLO Unit: EMDR in the Treatment of Psychological Trauma and How to Access…
A dark green background with a pale green border. A white rectangle text box in…
Text reads “LGBTQ+ Virtual Support & Consultation Group. May 8. 7 – 8 PM PT”…
Text reads "2024 Legislative Lobby Days Keynote Speaker. We cannot wait to share space with…
{kind=link}
{kind=link}